The Homebirth Cesarean project is a book-in-progress about mothers who planned home or birth center births but had to transport to the hospital for a Cesarean section. The project shines a light on the experiences of women who plan an out of hospital birth and then transfer, at some point in pregnancy or labor, for a cesarean. It also serves to honor the experiences of midwives and birth professionals, and to help both moms and midwives better navigate care.
The project was begun by a mother and midwife, Courtney Jarecki and Laurie Mednick,after their own Homebirth Cesarean experience. I asked them a few questions about their project. Here are their answers:
What about your personal experiences with birth brought you to your work on this project?
As a doula, childbirth educator, midwifery student and apprentice, Courtney was steeped in the world of birth for many years before becoming pregnant. She planned a homebirth and looked forward to bringing her baby into the world at home with her husband and dogs by her side. After over 50 hours of labor, she transported to the hospital during for a cesarean. The shock of this experience and the loss of her homebirth, shook Courtney deeply, as it does many women have homebirth cesareans
(HBC).
A homebirth cesarean is not just an unexpected birth outcome. It can be a shattering blow to a woman’s confidence, sense of self and identity,
her values, and it produces the kind of grief that only the loss of a deeply held dream can. As Libby, a HBC mom says, “The loss of my homebirth is as profound as the cesarean itself.”
Eight months after her daughter was born, Courtney sat down to discuss the birth with her midwives, specifically, to give them feedback. From that two hour conversation, Laurie’s interest was piqued. She invited Courtney back to discuss writing an article that would shine a light on these rarely discussed, heretofore unnamed births. Courtney proposed a book, and so the HBC project was born. What are some of the responses that you are getting from moms, midwives, and other maternity care
professionals?
In addition to co-authoring a book with the woman who was her midwife, Laurie Perron Mednick, Courtney started a closed Facebook support group for women processing their homebirth cesareans. The group began a little over a year ago with a handful of friends. It has since grown to over 900 members, including birth professionals who are interested in learning how to better care for HBC mothers.
Since 2011, Courtney and Laurie have interviewed over 150 mothers, midwives, and birth professionals. The feedback is overwhelmingly positive. The need for HBC to have a voice and to be represented is very present and deep. HBC mothers often feel like they no longer belong to the natural birth community, but neither do they fully identify with women who planned hospital births. They often say they feel like outcasts with no identity or community. The HBC project brings these women’s stories to the forefront and gives them a sense of belonging. As one mother
said during a storytelling event to raise funds for the HBC project, “I’m a librarian. And I like things to be categorized and have a place on the shelf. Because of HBC, I have a name, I have a category, and I finally found a place on the shelf.” The response from maternity care professionals has been very supportive. Courtney and Laurie have interviewed professionals ranging from therapists, midwives, OBs, to globally recognized birth experts such as Michel Odent and Sarah Buckley. All shared
their insights on the HBC experience, and many mentioned that there was a real gap in the birth discussion about these kinds of births. What form does the research take, what will the book contain, and are you planning on doing anything else with the information you gather?
The research for this book is rooted in Courtney and Laurie’s own HBC experience as mother and midwife, respectively. That experience guided
the research process, which includes phone, video, and email interviews.
The interviews are casual, with guiding questions that help elicit the participants’ views and experiences on HBC topics.
The book will feature several complete birth stories, each focusing on a different theme, including two stories from solely the partner’s perspective and one story from mom, partner and midwife. Overall, the book has roughly 15 chapters focusing on a different phase of the homebirth cesarean experience, including prenatal conversations, labor, transfer, the cesarean experience, hospital stay, and what it’s like after the first postpartum year. The appendix will contain helpful handouts for birth professionals and information for HBC families. Overall, the book provides first hand descriptions of what mothers have experienced, and information on how care providers can support women in these circumstances.
The research has also given rise to Courtney and Laurie
developing a series of classes for birth professionals. The first class offered
is called Speaking of Cesareans, and teaches midwives and
birth workers how to broach the transport and cesarean conversation with
clients prenatally. What sort of things
are birth professionals saying about homebirth cesareans? Sarah Buckley, she encouraged women to
submit their homebirth cesarean stories so they get heard and read as part of
the natural birth culture. She said, “People want to hear these stories, they
are beautiful.”
The idea that we need to hear more about HBCs in the current
birth discussion was echoed by Michel Odent who said: "If you look at the
research, more women want to give birth at home and these births are becoming
increasingly difficult. The HBC project is very important because there are
going to be more and more women in this situation who have ideals about
homebirth, who end up with a cesarean." What sort of things
are mothers saying about homebirth cesareans? Mothers often express that they feel like their births are
“dirty secrets” of the homebirth community, and that by having a cesarean, they
failed the natural childbirth movement they so deeply believed in. Mothers also
say that they felt woefully unprepared for the possibility of cesarean, and
that they believed that by talking about one prenatally, they might end up
causing one. This is magical thinking they now deeply regret. As one HBC mother
said, “Can you imagine if we didn’t teach pilots how to crash land because we
thought talking to them about it was too scary?” Before this project, a birth
that started at home and ended in the operating room didn’t even have a name.
Mothers, like the one mentioned above, say that they appreciate having a way to
describe their births that feels like it captures the hard work and intention
of homebirth while still voicing the surgical outcome. What is one thing you
want the public to know about homebirth cesareans? That they happen. They happen to all kinds of women in all kinds
of circumstances. They are real births and they deserve to be discussed and
honored.
__________________ Thank you to Courtney and Laurie for sharing this great project with me! For more information, please visit the HBC website: http://homebirthcesarean.com Click here to see the public Facebook page Twitter:https://twitter.com/HBCesarean#hbcesarean
Women's memories of their childbearing experiences stay with them for a lifetime
Too often, pregnant women seeking maternity care receive ill treatment that ranges from relatively subtle disrespect of their autonomy and dignity to outright abuse: physical assault, verbal insults, discrimination, abandonment, or detention in facilities for failure to pay.
The White Ribbon Alliance is working to break the silence surrounding ill treatment of women during pregnancy, childbirth, and postpartum:
The White Ribbon Alliance envisions a world in which a woman’s right to Respectful Maternity Care is embedded at all levels of all maternal health systems around the globe and that these rights are reflected in a sense of entitlement among women.
Interpersonal care that is disrespectful and abusive in nature to women before, during, and after birth is appalling because of the high value societies attach to motherhood and because we know the intense vulnerability of women during this time. All childbearing women need and deserve respectful care and protection of their autonomy and right to self‐determination; this includes special care to protect the mother‐baby pair as well as marginalized or highly vulnerable women (e.g., adolescents, ethnic minorities, and women living with physical or mental disabilities or HIV). Furthermore, disrespect and abuse during maternity care are a violation of women’s basic human rights.
You and your baby have the right to be treated with respect and dignity.
You have the right to be involved in and fully informed about care for yourself and your baby.
You have the right to be communicated with in a language and in terminology that you understand.
You have the right to informed consent and to informed refusal for any treatment, procedure or other aspect of care for yourself and your baby.
You and your baby have the right to receive care that enhances and optimizes the normal processes of pregnancy, birth and postpartum under a model known as the midwifery (or motherbaby) model of care.
You and your baby have the right to receive continuous support during labor and birth from those you choose.
You have the right to be offered drug-free comfort and pain-relief measures during labor and to have the benefits of these measures and the means of their use explained to you and to your companions.
You and your baby have the right to receive care consisting of evidence-based practices proven to be beneficial in supporting the normal physiology of labor, birth and postpartum.
You and your baby have the right to receive care that seeks to avoid potentially harmful procedures and practices.
You have the right to receive education concerning a healthy environment and disease prevention.
You have the right to receive education regarding responsible sexuality, family planning and women’s reproductive rights, as well as access to family planning options.
You have the right to receive supportive prenatal, intrapartum, postpartum and newborn care that addresses your physical and emotional health within the context of family relationships and your community environment.
You and your baby have the right to evidenced-based emergency treatment for life-threatening complications.
You and your baby have the right to be cared for by a small number of caregivers who collaborate across disciplinary, cultural and institutional boundaries and who provide consultations and facilitate transfers of care when necessary to appropriate institutions and specialists.
You have the right to be made aware of and to be shown how to access available community services for yourself and your baby.
You and your baby have the right to be cared for by practitioners with knowledge of and the skills to support breastfeeding.
You have the right to be educated concerning the benefits and the management of breastfeeding and to be shown how to breastfeed and how to maintain lactation, even if you and your baby must be separated for medical reasons.
You and your baby have the right to initiate breastfeeding within the first 30 minutes after birth, to remain together skin-to-skin for at least the first hour, to stay together 24 hours a day and to breastfeed on demand.
Your baby has the right to be given no artificial teats or pacifiers and to receive no food or drink other then breast milk, unless medically indicated.
You have the right to be referred to a breastfeeding support group, if available, upon discharge from the birthing facility.
A lot of people don't realize that public health is all around them. Public health is one of those things that is not noticed when it is working well, but generally when something goes wrong (a disease outbreak, an emergency, and so forth).
Public health is...
in the water you drink
in the seat belts and car seats that keep us safe in our cars
in your child's early education
in your workplace safety
in your neighborhood playgrounds and sidewalks
in your cafeterias
in your doctors' offices and pharmacies
in the clean air you breathe
... and more!
Public Health's mission is to help every individual to attain a complete state of physical, mental, and social well-being. Health is not merely the absence of disease or infirmity. We work at the population level, to improve the well-being of communities as a whole, not just one individual at a time.
This year's NPHW's theme is ROI - Return on Investment
The U.S. spends far more on health care than any other country, with such costs rising ten-fold from 1980 to 2010.
Did you know that only 2% of our U.S. healthcare dollars are spent on public health?
But we get BIG returns. Public health initiatives save millions of dollars and millions of lives! The more we focus on PREVENTION, the bigger the health impact.
Routine childhood immunizations save $9.9 million in direct health care costs, save 33,000 lives and prevent 14 million cases of disease.
A $52 investment in a child safety seat prevents $2,200 in medical costs, resulting in a return of $42 for every $1 invested. Similarly, a $12 investment in a child’s bicycle helmet can prevent $580 in medical costs, resulting in a return of $48 for every $1 invested.
The cost of providing dental care for children enrolled in Medicaid and living in communities without fluoridation is twice as high as for children who receive the oral health benefits of drinking water fluoridation.
Each 10 percent increase in local public health spending contributes to a 6.9 percent decrease in infant deaths, a 3.2 percent decrease in cardiovascular deaths, a 1.4 percent decrease in deaths due to diabetes, and a 1.1 percent decrease in cancer deaths.
Every year, newborn screening efforts test nearly every baby born in the U.S. for health conditions that — if detected early enough — can be treated in time to prevent developmental problems, disability and death. For example, testing the 4 million infants born every year for congenital hypothyroidism costs $5 per newborn and prevents 160 cases of intellectual disability.
By 2020, the direct benefits of the federal Clean Air Act will have reached almost $2 trillion, much more than the $65 billion it will have cost to implement the law. About 85 percent of the $2 trillion is attributable to decreases in premature death and illness related to air pollution.
Citing the protective health benefits of breastfeeding, research finds that a minimum of $3.6 billion could be saved if more women began and continued to breastfeed their newborns through 6 months of age.
Whether it’s through research, data collection, health education, policy change or direct services, public health lays the foundations and creates the conditions that put the healthy choice well within reach.
Would you like a little more information on how public health works? Here are some great visuals:
These are all the groups that public health works through - the government, universities, the media, business, community organizations, and health care
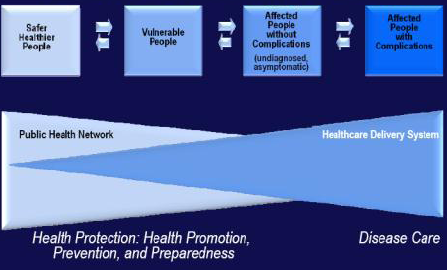
This shows how public health works from one end of things - protection, promotion, prevention, preparedness for safer healthier people - and overlaps somewhat with the healthcare delivery system - disease care for affected persons.
Your health is affected by your health behaviors, the clinical care you receive, the physical environment in which you live, and social and economic factors. Social and economic factors have the largest impact (40%), and physical environment has the least (10%), but they all play a role in your health outcomes.